Let me be honest about something I've been doing for years. A patient comes in post-op, or after a strain, and I need to document their knee flexion. I eyeball it. Maybe I grab a goniometer, hold it steady while the patient holds their position, squint at the dial, and write down a number, knowing full well that the next clinician to see that patient might get a reading five or ten degrees different for no good reason. We've all done it. It's not that we're bad clinicians. It's that we've been working with century-old measurement tools for a problem that now has a genuinely better solution.
That solution is AI-powered computer vision range of motion assessment, and after spending real time with EverEx's technology, I want to make the case that this isn't just a shiny gadget, it's a meaningful clinical upgrade.
The dirty secret of goniometry
Ask any PT to define "normal" goniometer reliability and you'll get an uncomfortable pause. The inter-rater reliability of standard goniometry for most joints is moderate at best. Studies have put inter-rater variability at ±5–10° for the knee, and worse for complex joints like the shoulder or wrist. That's a meaningful spread when you're trying to determine whether a patient has plateaued, whether they've met discharge criteria, or whether a post-surgical recovery is on track.
"We've been asking patients to hold uncomfortable positions while we fiddle with a plastic protractor, pretending the result is objective data. It is not."
Inclinometers help, but they add cost, require calibration, and still depend heavily on clinician positioning and patient stability. Visual estimation — let's just call it what it is, eyeballing — is even worse, with studies showing inter-rater differences of 10–15° on common joints. For documenting treatment progress, justifying continued care to insurers, or communicating across a care team, that's simply not good enough.
The stakes are real. If I document 95° of knee flexion today and my colleague documents 105° next week, the chart suggests ten degrees of improvement that may not exist. Or it suggests no progress when there actually was some. Either way, the clinical picture is distorted — and in a value-based care environment, distorted data has consequences.
±10°
Typical inter-rater goniometer variability
27
Joints assessed by EverEx AI in a single session
0.90
ICC reliability for lower-limb alignment (EverEx)
What computer vision actually does differently
Modern AI pose estimation works by detecting anatomical keypoints from camera footage — no markers, no wires, no calibration rigs. The algorithm identifies joint centers, tracks their position frame by frame, and calculates the angles between body segments in real time. The patient just moves normally. That’s a fundamentally different kind of data. Instead of “knee flexion was approximately 95° at peak,” you get “knee flexion peaked at 94.3°.”
The EverEx model: built with clinicians, validated against gold standards
What drew me to EverEx specifically is how their model was developed. The AI wasn’t trained solely on generic human pose datasets scraped from the internet. Several doctors, physical therapists, and musculoskeletal clinicians were directly involved in teaching and refining the model — annotating clinical movement patterns, flagging compensations, and helping the algorithm understand the difference between a real range of motion assessment and a faulty positioning angle.
The model tracks 24 anatomical keypoints across 27 joints, covering the full kinetic chain from the cervical spine to the ankle. That’s a clinically meaningful scope — it means you can assess the shoulder complex while simultaneously watching what the trunk and hip are doing, which is exactly the kind of whole-body view that separates good PT assessment from checkbox documentation.
Validated against radiographic imaging (Diagnostics, 2025)
A prospective study of 72 participants compared EverEx’s MORA Vu software against X-ray gold standards for cervical and lower-limb alignment. Forward head posture showed strong correlation with the craniovertebral angle (r = −0.712), and digital hip–knee–ankle angle correlated strongly with radiographic measurement (r = 0.754). Inter-rater reliability was excellent: ICC 0.84 for cervical, 0.90 for lower limb.
Verified against Vicon 3D motion capture (Medicina, 2026)
A concurrent validation study compared EverEx’s single-camera markerless system against both an 8-camera Theia3D system and the Vicon marker-based gold standard. The single-camera approach demonstrated good-to-excellent reliability for spatiotemporal gait parameters and strong agreement in sagittal-plane hip and knee kinematics — matching multi-camera performance at a fraction of the cost and complexity.
Faster, smoother, and more accurate than open-source alternatives
I know what some of you are thinking: “Can’t I just set up OpenPose or MediaPipe on a laptop and do the same thing?” Technically, sort of. Practically, no.
Open-source pose estimation models were designed for general human pose detection — think video games, fitness apps, surveillance. They weren’t trained on clinical populations, on patients with altered movement patterns, on people who walk with a Trendelenburg gait or hold their arm in a sling. The EverEx model was pretrained on a dataset of over 87,000 images containing 121,000+ annotated individuals performing clinical and functional movements. The accuracy difference is real and visible.
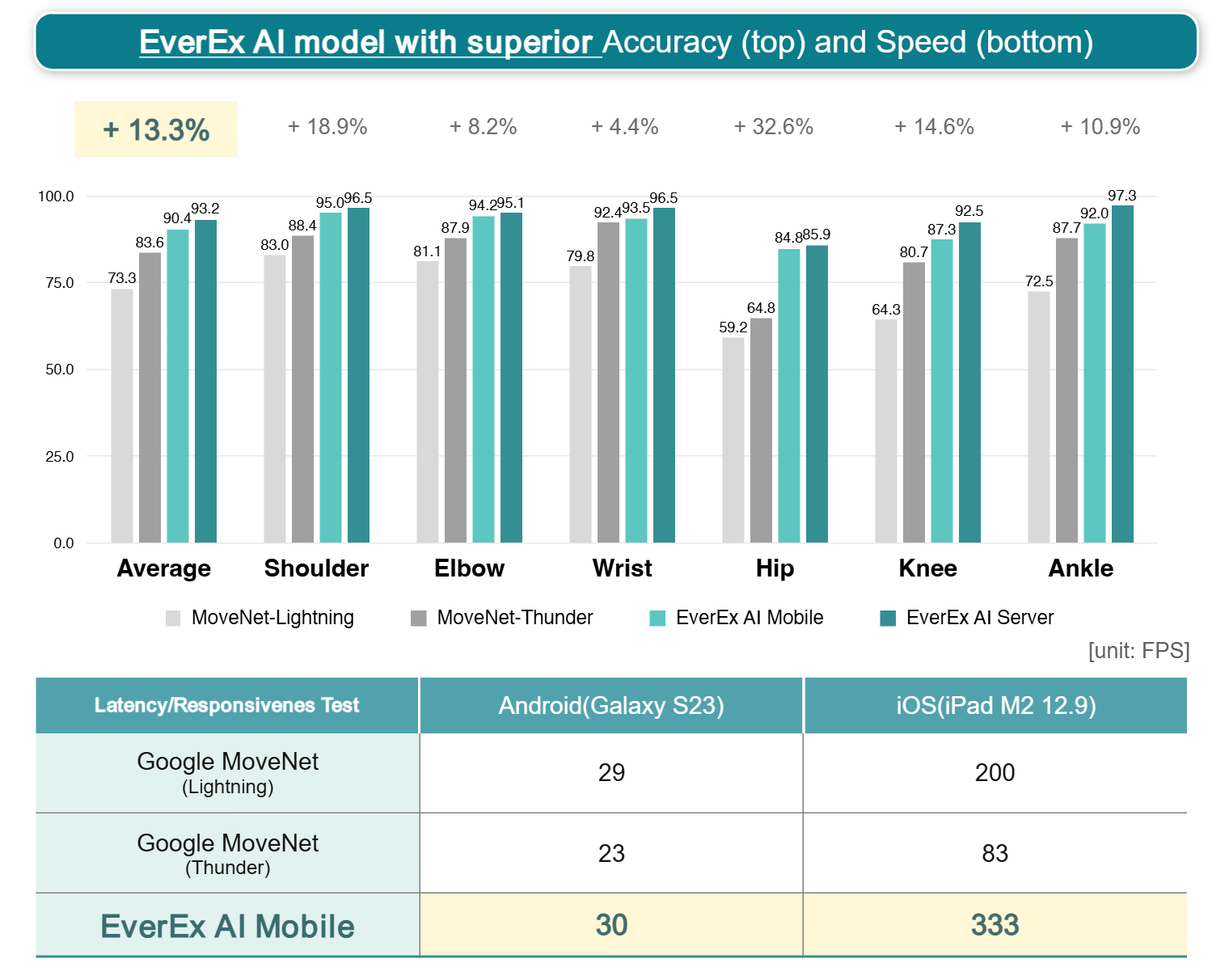
In head-to-head benchmarks against Google’s MoveNet (the current leading open-source option), EverEx’s mobile model delivers +13.3% higher average accuracy across joint types — with particularly large gains at the hip (+32.6%) and shoulder (+18.9%), which happen to be the two joints PT clinicians assess most. On speed, the EverEx model runs at 333 FPS on an iPad M2 compared to 83–200 FPS for MoveNet variants. That’s not just a spec-sheet win — it means the overlay is genuinely smooth and real-time during dynamic movements, not stuttering and catching up.
See it in action
Words only go so far. Watch EverEx's computer vision ROM in real-time — from camera input to final measurement in under two seconds.
What this means for your daily practice
Here’s what changes when you have reliable, objective ROM data that’s fast to collect and consistent across clinicians:
Documentation becomes defensible
When every session produces an objective angle trace rather than a clinician estimate, your progress notes reflect actual patient function. Insurers, referring physicians, and care teams get data they can act on.
Plateaus become visible — and real
If a patient has genuinely stopped improving, the data will show it. But equally, if they’ve made subtle gains that a goniometer snap-measurement would miss, the full range trace will capture them. That’s both better for the patient and better for the clinical relationship.
Compensatory movements stop hiding
This is the one that excites me most. A patient can hit a “normal” end-range value while compensating through the spine, the hip, the trunk — and traditional ROM measurement will never catch it. Computer vision that tracks 27 joints simultaneously makes those substitutions visible in the data. You’re not just measuring the target joint; you’re assessing movement quality.
Handoffs improve
When I document my patient’s shoulder abduction as 148° so will the next clinician using our tool. That’s not how it works with eyeballed estimates written on a paper form.
A note on the research base: The two published validation studies cited above used EverEx technology specifically — comparing it against cervical and lower-limb radiographs (Diagnostics, 2025) and against Vicon 3D marker-based motion capture (Medicina, 2026). These aren’t cherry-picked pilot results. They’re peer-reviewed, IRB-approved studies with standard statistical methods, and the results hold up. ICC values in the 0.84–0.90 range for inter-rater reliability is the bar you’d want any clinical measurement tool to clear.
The honest limitations
I’m not going to pretend this is a perfect solution. The validation research on AI-based ROM is still maturing. Ankle kinematics in particular remain a challenge for single-camera systems due to the complex tri-planar motion at that joint — the EverEx gait study acknowledged this directly, which I respect. Real-world clinical settings have more variation in lighting, clothing, and patient body habitus than the controlled environments where these systems are validated.
What I will say is this: the existing evidence compares favorably to the existing evidence base for the tools we’re already using. Goniometry has an enormous published literature, but a lot of it shows mediocre reliability numbers that we’ve collectively decided to live with. The question isn’t whether AI ROM is perfect. It’s whether it’s better than what we have, and for most of the assessments we do most of the time, I think it demonstrably is.
My take
I became a physical therapist because I believe in the science of movement and function. The ability to measure movement accurately — to actually see what’s happening at 27 joints simultaneously, in real time, with data that’s reliable enough to track week over week — is something I would have found incredible when I was in PT school. The fact that it now lives in a smartphone-based system that a clinician can deploy in an outpatient clinic without a dedicated lab space or a motion capture technician is genuinely remarkable.
We owe our patients accurate data. We owe our documentation the rigor we’d want applied to any other clinical measurement. Computer vision AI ROM is finally at a point where it can deliver both. That’s worth getting excited about.